Exercise is the best treatment for non-specific low back pain but which type of exercise is the best to use and when?
There are numerous clinical practice guidelines which recommend exercise as the first line treatment for non-specific low back pain and rightly so. Numerous high quality studies have highlighted this to be true including a recent Cochrane systematic review.
The challenge is, at the moment it’s very difficult for us to say which type of exercise is the most effective for treating the condition. This is because a systematic review compares two treatments at one time and don’t allow for full analysis of trials investigating multiple treatment groups within studies.
Calculate Which Exercise Your Patient Needs
This limitation was known by the team which completed the recent systematic review (linked to above) knew this and have taken their results one step further by performing a network meta-analysis. this means multiple treatments can be compared simultaneously and consider wider variables which could have an effect on outcomes.
Therefore the specific research question for this network meta-analysis was “What are the effects of specific types of exercise treatments on pain intensity and functional limitation outcomes for adults with chronic low back pain?”
Methods
This study adhered to the network meta-analysis PRISMA guidance.
The search criteria was the same as the one used in the initial Cochrane review and involved searching nine databases with a comprehensive search strategy which is available in full within appendix 1 & 2 of the initial systematic review protocol.
The inclusion and exclusion criteria is also available in full within the original protocol but in summary the PICO of the review is as follows:
- P – adults with chronic non-specific low back pain for 12 weeks or more
- I – Exercise treatments prescribed/planned by a healthcare professional. Involved specific activities, postures / movements with a goal to improve low back pain
- C – placebo, education, manual therapy, back school, electrotherapy, mixed treatment not including exercise, psychological therapy, pharmacological therapy and relaxation
- O – pain intensity (VAS / numerical) and back related functional limitations (RMDQ, ODI etc)
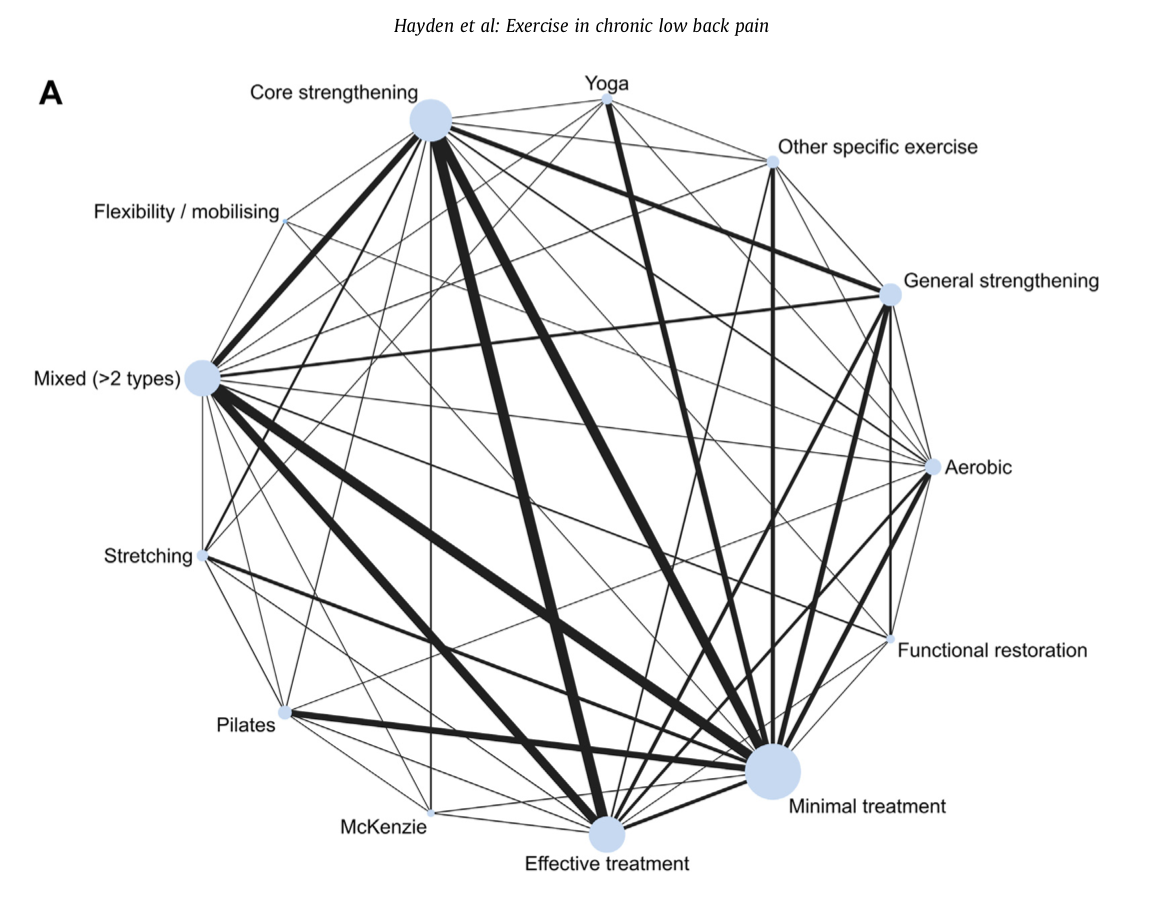
Exercise interventions were divided into 11 categories; core strengthening / motor control, mixed exercise, general strengthening, aerobic, pilates, stretching, yoga, McKenzie, functional restoration, flexibility and other specific exercises.
Results – Included Study Summary
In total 249 RCTs (n=24, 486) were included within the review and 217 (n=20, 969) provided sufficient data to form the network meta-analysis. Most of the trials included (56%) took place in healthcare settings with the rest taking place in general population or mixed settings.
The number of participants included from trials ranged from 10-722 with a median sample size of 70. the mean pain severity score was 44/100 on the VAS. The median time point of the short-term follow up was 12 weeks.
In terms of quality of the studies there were multiple concerns particularly with selection bias which was present in half of the studies. Additionally 79% of the studies has issues with performance bias and a similar amount with concerns of detection and reporting bias. All of these reduce the confidence of the findings of the review.
There were additional concerns with the definitions used to describe the exercises used within the studies as well as standardisation of treatment approach. The most common exercise investigated was core exercise (30%) followed by mixed exercise (3+ types) and general strengthening.
Supervised group exercise was the most common delivery method (40%) with 39% being delivered at home with supervision. Only 19% were deemed to be an individualised approach. The median time of the treatment was 12 hours delivered over a median of 8 weeks. 57% of interventions were combined with additional intervention including exercise, education and manual/electrotherapy.
Results – Which Exercise is Best?
The overall certainty of the evidence for both pain intensity and functional limitations was moderate overall. This is because of the bias found in the included evidence as well as lack of clarity around intervention definitions and incomplete reporting outcomes.
Pain Intensity
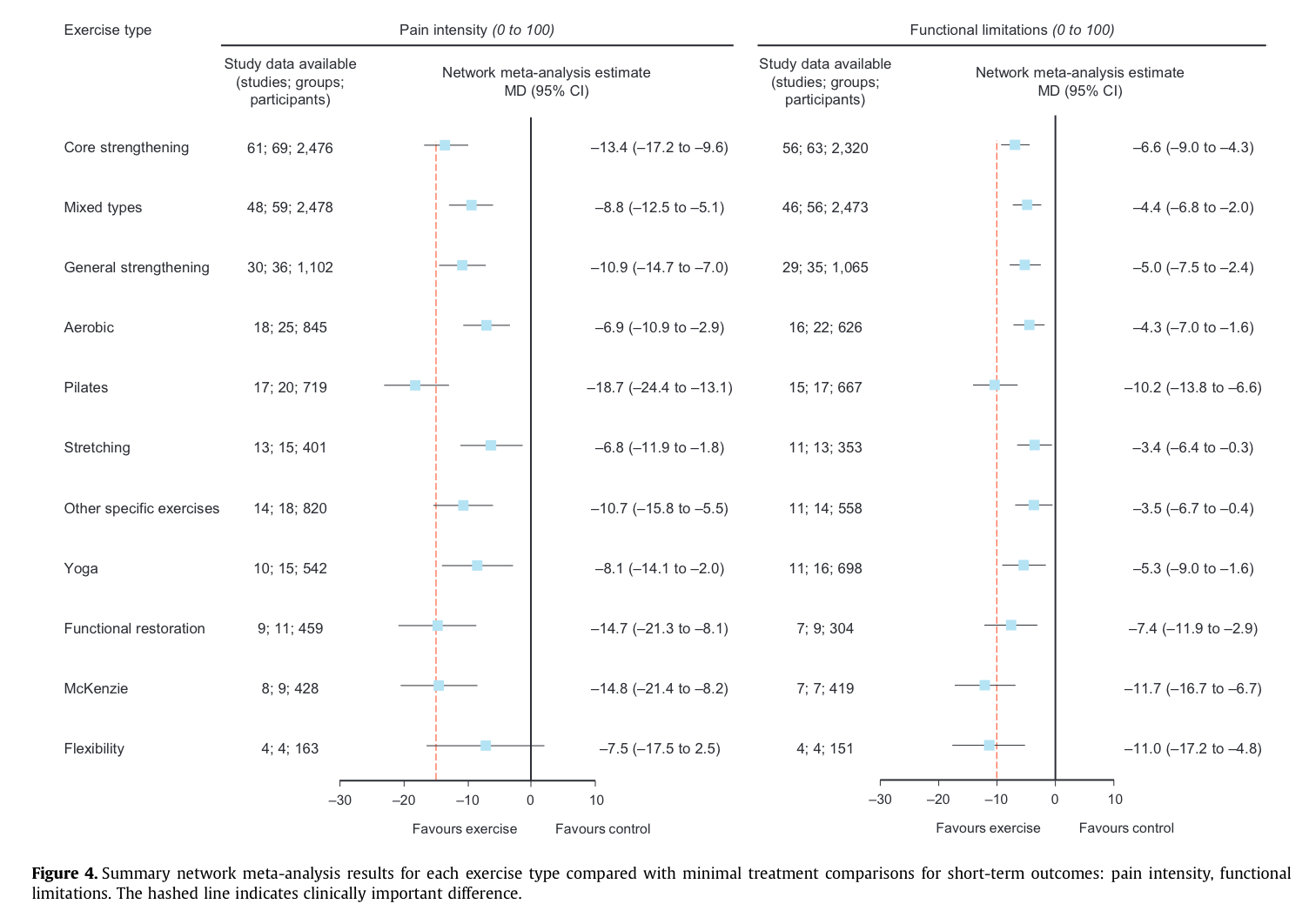
In total 198 trials measured pain intensity and the most effective type of exercise for reducing pain intensity was Pilates followed by the McKenzie method and functional exercises all improving VAS score between ~20-40 points.
The network meta-analysis, which included 81 potential treatment combinations demonstrates that Pilates was the most effective treatment option when compared to all other conservative treatments.
Functional Limitations
In total 187 trials included data about functional limitations. The results of the network meta-analysis show that McKenzie, Pilates and flexibility exercises were shown to be most effective at improving functional limitations.
The results of the meta-analysis are shown in full for all the exercise categories, are shown below.
Implications for Clinical Practice
This network meta-analysis provides further support for exercise treatment being effective at treating non-specific low back pain. Most exercise types are more effective than manual therapy / electrotherapy and dose and intensity should be based on likelihood of patient uptake. Overall McKenzie, Pilates and functional exercise are the most effective forms of exercise for reducing pain and functional limitations.
