The body is complex, as few, tempted to read on would dispute. Starting any piece by reinforcing the complexity of the body seems fairly redundant, yet, within this complexity patterns may be discernible, and perhaps certain behaviours may be considered predictable. Lets consider movement and the patterns and shapes within it.
The many shapes the body forms are open to interpretation from the observer, as seen in body language (Gelder, 2006) or the discursive movement of dance (Harman, 2007). In the movement sciences, these external patterns inform on the latent goings-on, the hidden processes of neurophysiology, metabolism and the other systems at work below the surface.
Movement solutions to movement problems
The observation of movement also supplies insight on how the body as a whole can problem solve when barriers to task achievement arise. If a region lacks extensibility, force production qualities or is in pain, a ‘movement solution’ can be found in order to still get through the day or just the next 5 minutes.
The barrier to movement – limited dorsi flexion
A recent article by Bell-Jenje et al. (2015) lends support to the idea of the body as a problem solving device/machine, accommodating for deficits in regional task achievement (lack of dorsi flexion) by asking for greater contributions from elsewhere. This study identified how pain free females with limited dorsiflexion range (<17 degrees) increased their use of hip adduction during the completion of step down task. The lack of sufficient sagittal range at the ankle was seen to be managed in the frontal plane at the hip. The authors go on to comment on the associations between hip adduction, knee valgus and the heightened injury risk ascribed to these dynamic alignments within this population. The short term solution to this particular barrier to movement may carry long term injury associated problems.
Dorsiflexion restriction and valgus, is it predictable? No.
The same solution is sometimes found to the same problem. Vesci et al. (2007) saw limited dorsiflexion to be accompanied by increased knee valgus in a double leg squat. However, it is also apparent the body may solve the issue of limited dorsiflexion in other ways. People move differently and solve their movement conundrums in different ways.
Many solutions to the same problem
In the case of a limitation in dorsiflexion individuals might also increase the use of mid-foot pronation, lateral rotation of the tibia and flexion of the hip. All are commonly seen, clinically. At the lumbar region all outcomes seem possible, as extension and flexion are common, as is rotation when the ankle restriction is unilateral in nature.
So, what is predictable?
What seems predictable is that a short term solution will be found by the body, yet the compensatory pattern to be used is the main question. Assessing range of motion of the ankle informs us a restriction may be present and therefore the likelihood of a compensatory strategy is highly likely. We have found a barrier but not the individual’s adopted solution. To find this compensation we need to assess movement in a multi-joint approach, revealing exactly where the problem solving strategy manifests. If this strategy cannot be prevented from occurring during a test of cognitive control it may be classified as uncontrolled, unpreventable (Mottram & Comerford, 2008). If this movement cannot be prevented it is likely to always appear, lowering movement variability in joint coupling, and elevating overuse risk (Hamill et al., 2012).
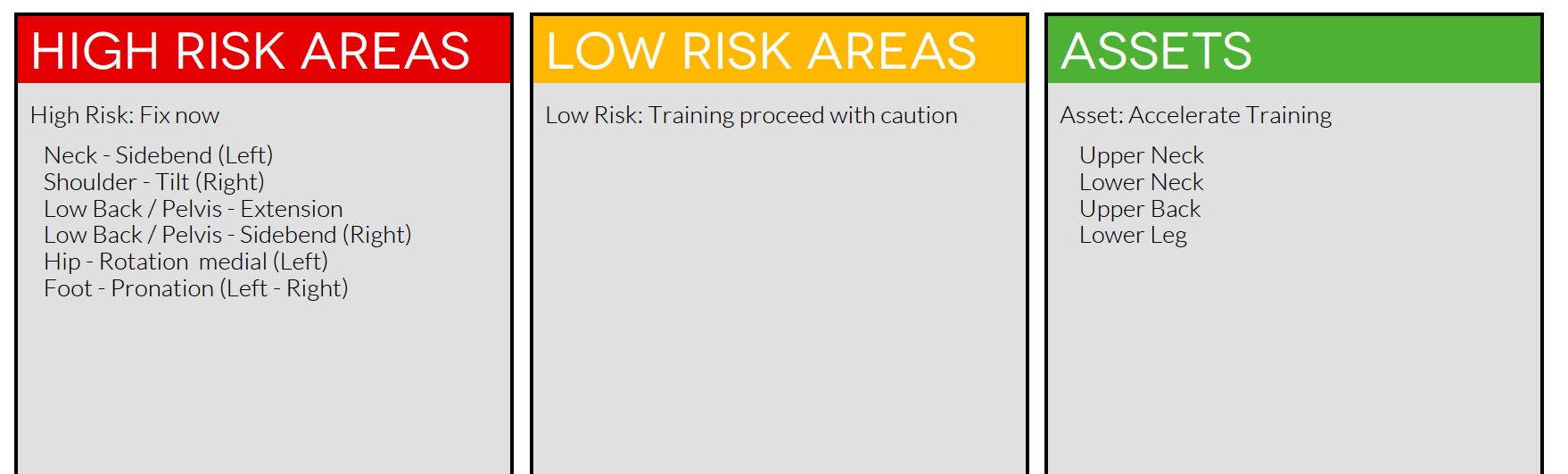
Finding the barriers to movement is insightful. We must identify the strategies to solve the problems these barriers create with risk related to movement and movement health. One way of doing this is with The Performance Matrix online screening system which details compensations with Site, Direction & Threshold.
Check out the Performance Matrix Here
References
- Bell-Jenje T, et al., (2015). The association between loss of ankle dorsiflexion range of movement, and hip adduction and internal rotation during a step down test, Manual Therapy (2015), http://dx.doi.org/10.1016/j.math.2015.09.010
- De Gelder, B. (2006). Towards the neurobiology of emotional body language. Nature Reviews Neuroscience, 7(3), 242-249.
- Hamill, J., Palmer, C., & Van Emmerik, R. E. (2012). Coordinative variability and overuse injury. BMC Sports Science, Medicine and Rehabilitation, 4(1), 45
- Harman, R. (2007). “Critical teacher education in urban contexts: Discursive dance of a middle school teacher.” Language and Education 21.1 (2007): 31-45.
- Mottram, S., & Comerford, M. (2008). A new perspective on risk assessment. Physical Therapy in Sport, 9(1), 40-51.
- Vesci BJ, Padua DA, Bell DR, Strickland LJ, Guskiewicz KM. (2007). Influence of hip muscle strength, flexibility of hip and ankle musculature, and hip muscle activation on dynamic knee valgus motion during a double-legged squat. J Athl Train;42(2 Suppl):S-83.