Here we consider the influencing factors that increase the probability of sustaining a stress fracture to the metatarsals. The topic is addressed with regards to the movement management system that is The Performance Matrix, powering the TPM Active, TPM Elite and TPM Active philosophies.
First, a little background
The metatarsals provide a broad surface for load sharing on the foot’s plantar surface, forming the connection for both phalangeal and mid-foot articulations. Stress fractures to these structures are common, certainly within particular groups who endure large volumes of weight bearing (Cakir et al., 2014). Milgrom et al, (1992) showed that out of a total of 184 stress fractures, 7.6% of were of the metatarsals within a group of 205 military personnel.
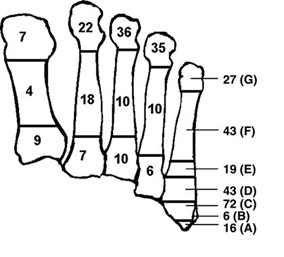
Figure 1: distribution of metatarsal fractures according to their location (Cakir et al., 2011)
Risk factors
A number of risk factor have been identified for this injury. The perspective taken here is that of an interactive and accumulative effect brought about by a number of issues including those relating to training, fatigue status, hormonal state, contact surface and whole body movement quality and others. Firstly, we consider volume of training.
Why volume should be monitored and gently increased
Stress fractures can be considered as either as a normal system failing to meet the demands on that system (fatigue stress fracture) such as when exposed to high volumes of repetitive loading (>15 hours a week) or a compromised system failing to meet a constant demand (Insufficiency stress fracture). An increase in volume of ground contacts associated with running leads to a disruption of the usual cycle of bone remodelling. Osteoclast activity increases (‘breaking down bone’) whilst there is a lag in the activity of osteoblasts (‘building bone’). This change to the system can increase the chance of a stress fracture. This is suggested to a risk if volume increases more than 10% in a week and is compounded if volume of running already exceeds >15 hours a week.
Who is at risk?
To profile an individual at higher risk for this injury we would identify a female with low body fat percentage, involved in high volume of running. They may have recently increased their volume or be at a peak volume of running in preparation for an upcoming event. The knowledge of this important event may itself be a stressor to the system, increasing fatigue, which in turn may also increase risk. One way in which this may operate is the following example. The runner may begin to experience discomfort in the foot, indicative of a problem. Rather than resting the runner sticks to their programme as the race ‘really matters’. There is now an interaction between the stress of the upcoming race, the worry of the foot and the concern over the need to maintain the running volume.
Why the female runner?
One very simple reason is the size of bone in female compared to male feet. On average, the female foot will be smaller. Additionally, when body fat is very low (<12% for females) there is a risk of disruption to the monthly cycle, indicative of a change in hormonal status. The hormones involved are closely related to bone density, therefore heightening fracture risk. If the female runner is also deficient in vitamin D, iron and/or calcium bone health is further compromised.
Fatigue?
The accumulative effect of fatigue is seen to problematic. It reduces the body’s natural self-monitoring system or CCTV typically called proprioception, which tells us about our movement. Also, fatigue is seen to reduce the ability to absorb shock efficiently as an event progresses, increasing pressure below the mid-foot (where the metatarsals lie) (Weist et al., 2004).
Surface, Shoe, Style?
It appears it is the change in surface that can be an issue. Those accommodated to a softer surface may experience issues when switching to harder running environments and vice versa. This is probably related to gaining familiarity with efficiently ‘hitting’ a novel surface and problems may arise before this solution is found. The same can be considered for shoe type and running style (how you hit the floor- heel-toe or mid-fore foot) – it appears to the transition to the new that carries risk; although old shoes (worn out) are also associated to increased risk.
OK- what about stress fractures, movement quality & The Performance Matrix?
We believe everyone in the world should have their movement assessed in order to ensure they are free of what we call uncontrolled movement (Comerford & Mottram, 2012). This definitely includes runners whether male or female but we don’t just look at their feet or even just their legs. With regards to stress fracture here’s a few thoughts why;
 In distance events, people typically aim to run in a straight line. During movement analysis we might discover somebody really struggles not to allow their pelvis and low back swing/rotate from side to side- they just can’t stop it happening. During running this could be trouble for the feet. If the hips consistently rotate in this way the runner’s feet, which are aiming to keep the runner in a straight line and are loaded with a multiple of body weight in each step, are consistently twisted. Combined with some of the factors already mentioned this might just be a stress, placed a direction in which the metatarsals are not their most robust, to start the process of injury.
In distance events, people typically aim to run in a straight line. During movement analysis we might discover somebody really struggles not to allow their pelvis and low back swing/rotate from side to side- they just can’t stop it happening. During running this could be trouble for the feet. If the hips consistently rotate in this way the runner’s feet, which are aiming to keep the runner in a straight line and are loaded with a multiple of body weight in each step, are consistently twisted. Combined with some of the factors already mentioned this might just be a stress, placed a direction in which the metatarsals are not their most robust, to start the process of injury.
This is just one combination of a movement issue in one region producing a potential issue in another. Finally, on the topic stress fractures, previous injuries are still the biggest predictor for re-injury. We believe these injuries leave a movement fault ‘signature’ that linger once the original injury has gone which then leads to more problems. The Performance Matrix goes looking for these signs, and helps you fix them before find re-injury is becoming a regular part of your training year.
The topic is complicated as many factors increase risk. One thing we can find and fix is your movement. Addressing the other concerns mentioned above and working on your movement quality is a course of action to keep you doing the things you like, love or to keep allowing you to have the things that doing this gives you.
References
Cakir H, Van Vlit-Koppert ST, Van Lieshout EM, De Vries MR, Van Der Elst M, Schepers T, Demographics and outcome of metatarsal fractures. Archives of Orthopaedic and Trauma Surgery (2011); 131: 241-245.
Comerford, M. & Mottram, S. (2012). Kinetic Control: The Management of Uncontrolled Movement. Australia: Elsevier.
Milgrom C, Finestone A, Shlamkovitch N, Wosk J, Laor A, Voloshin A, Eldad A – Clinical Orthopaedics and Related Research 1992 Aug; (281):189-192 [A1]
Prevention of overuse injuries of the foot by improved shoe shock attenuation Weist R, Eils E, Rosenbaum D. The influence of muscle fatigue on electromyogram and plantar pressure patterns as an explanation for the incidence of metatarsal stress fractures. Am J Sports Med 2004;32(8):1893–8.
Put multi-joint assessment in your practice using our range of movement analysis tools including The Running Matrix
