We know that back pain is the leading cause of disability worldwide with over half a billion people living with back pain every day. Around 75% of people will experience at least one episode of back pain during their lifetime and a large proportion (~25%) go on to develop chronic pain.
Many patients present in primary care for initial treatment of thier back pain and a stratified approach to managing care has been proven effective at reducing the number of patients which go on to develop chronic issues.
Explore Stratified Care for LBP
The evidence for a stratified approach has been well studied in European health systems and proven to be effective however a US based study published in 2018 was unsuccessful when using the stratified approach. A new study published this week has revisited this in a US population.
The aim of the TARGET trial was to test if implementation of a risk-stratificatied approach to management of back pain in primary care would result in lower results of chronic low back pain and improved self-reported disability in the USA.
Methods
The TARGET trial was a multi-site cluster randomised controlled trial with a 1:1 allocation ration. The cluster sites were 5 primary care clinics in the US; UPMC, BMC, JHM, IH and MUSC. These clinics were randomised into two groups – one being usual care and the other being usual care + psychologically informed physical therapy.
 Patients who were 18 years or older who presented to participating primary care clinics with a primary complain of acute low back pain were eligible for participation within the trial. If pain had been present for more than 3 months, or if pain had prevented daily activites more than every other day participants were excluded as this classified them as having chronic symptoms.
Patients who were 18 years or older who presented to participating primary care clinics with a primary complain of acute low back pain were eligible for participation within the trial. If pain had been present for more than 3 months, or if pain had prevented daily activites more than every other day participants were excluded as this classified them as having chronic symptoms.
All remaining participants then completed the STarTBack Tool which divided the participants into a high-risk group (a score of 4 or more), medium group or low risk group. These high-risk patients patients were entered into the trial and randomised into either ususal care or usual care + psychologically informed physical therapy.
The trial was pragmatic in nature which meant that the standardisation of the psychologically informed physical therapy was not closely monitored however a treatment checklist was developed and used by the clinicians involved in the trial. This clearly has implications for the results however is more representative of variable practice in real clinical situations on a daily basis.
The primary outcome for the study were patient reported transition from acute to chronic low back pain and back pain related disability at six months (ODI). Secondary outcomes was medical utilisation over 12 months from initial assessment measured by outpatient visits, imaging requests, pain procedures and hospital admissions.
The protocol for the trial is available to read in full on pubmed.
Results & Clinical Importance
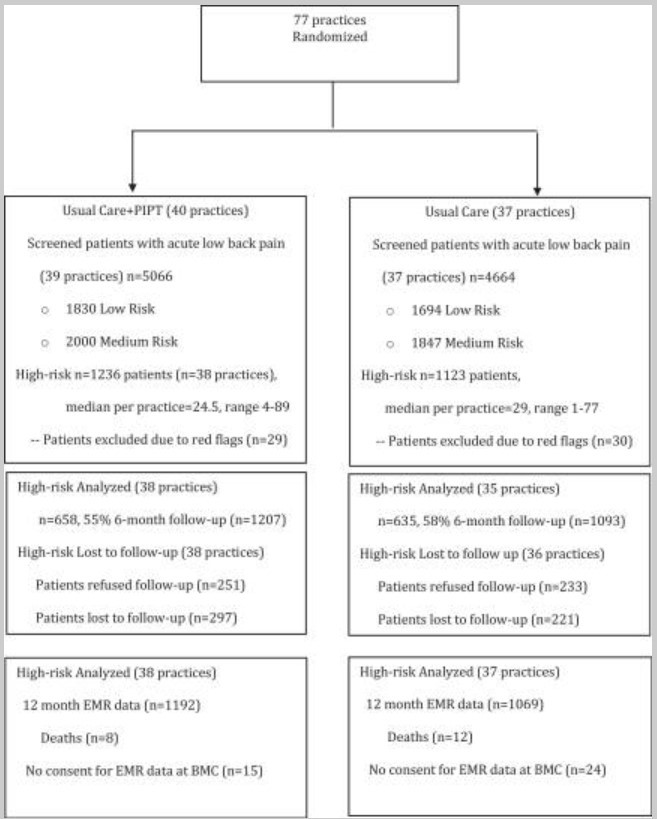
In total 77 clincials were randomised across 4 sites recruited 2,300 participants with 1207 in the intervention group and 1093 in the control group. Interestingly during the screening phase for eligibility 50% of patients seen already had chronic back pain which exceeds current estimates in the US. During this screening phase 36% were low risk, 40% medium risk and 55% high risk for developing persistent (and therefore chronic) back pain.
A lot has been said about the opioid epidemic in the United States and at the first visit 22-25% of the high risk group recieved opioids, 40% for muscle relaxants (non-specific) and 30% for NSAIDs – all of which we know to be largely ineffective for back pain if used for longer than the very early stages of an acute episode. At 1 year 8% continued to take opiates.
Essential Concepts of Analgesia
Considering only 57% of participants in the intervention groups had a referral to physio or physio + psychological intervention but 25% recieved opiates is an indication of overreliance on pain killers – it’s too easy to get the prescription prior to seeking alternative means of pain management first. This is contrary to all recent clinical guidelines for low back pain.
Only 5% of participants at the initial consultation recieved referral to a non-medical back pain specialist which is interesting and unfortuntately the subgroup analysis of these patients isn’t granular enough to analyse further.
At the 6-month point around half of the patients in both groups reported transitioning to chronic pain with 70% having their daily lives affected. This is demonstrated in the bar chart below.
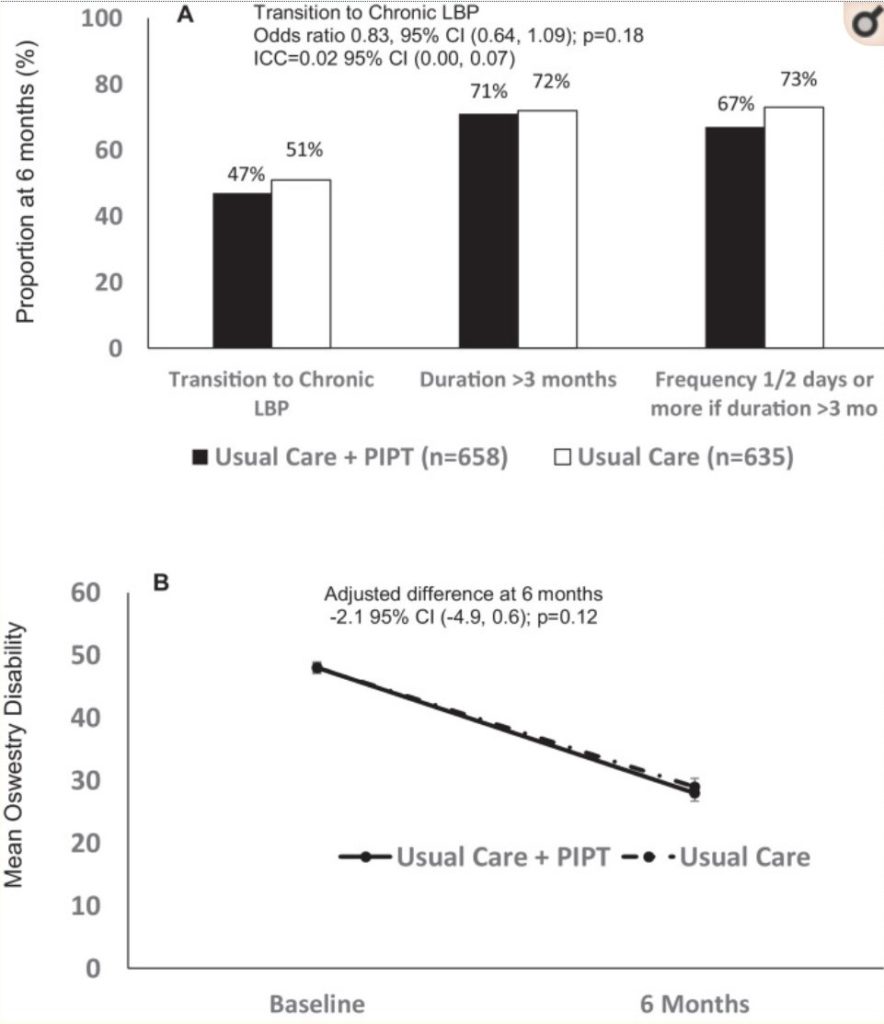
However, there was an overall reducion in number of participants with severe disability according to ODI suggesting some success with the interventions, particularly the psychologically informed treatment group. However this success did not reach clinical or statistical significance for either group at 6 or 12 months. It is quite possible that the participants who transitioned to chronic pain adapted their lifestyles to live with the pain as much as possible therefore reducing their ODI scores.
In summary 51% of participants in the intervention arm and 48% of in the control arm transitioned to chronic back pain indicating no significant difference in outcome between the two groups. The change in ODI score is likely due to individuals adapating their lives to living with chronic pain however this is unclear given the detail provided within the study.
Stratified care for low back pain has been proven to be effective in European health systems but clearly this can’t be said for the United States of America. There are likely other cultural and economic factors at play here such as insurance, access to specialists and the current over reliance on opiates.