The International Framework for the examination of the cervical region for potential vascular pathologies of the neck prior to manual therapy has been updated. We’ve summed up the key clinical take homes for you.
The Framework is designed to provide guidance for the assessment of the C-Spine for potential vascular pathologies of the neck in advance of planned mobilisation, manipulation and exercise. The first edition was published in 2012 and, although scheduled for revision in 2017, an update has now been published.
The reason why we need this document is that since the beginning of manual therapy there has been a history of neurovascular patient safety incidents related to the use of the therapy as well as more recently, the emergence of vascular masqueraders. These are arterial pathologies which can potentially present as msk pain and dysfunction. Therefore the aim of this document is to increase clinician understanding of risk and pathology to ensure safety.
Take Home Messages
- Incidents are rare however they are not impossible or unheard of therefore adherence to this framework is strongly recommended
- Cervical Artery Dysfunction (CAD) has been replaced with Vascular Pathologies of the Neck
- Provocative positional testing is not recommended instead clinicians should form an index of suspicion based on robust subjective assessment
- A single test does not exist to test a vascular hypothesis therefore understanding patient presentation is essential
- The aim of the document is not to provide you with a protocol to adhere to but to increase clinician understanding of risk and pathology to ensure safe practice
- The rate of vertebral artery (VA) dissections in the general population is estimated to be 0.75-2.9 per 100,000.
- Internal carotid artery (ICA) dissections occur 3-5 x more frequently.
- The majority of serious adverse events associated with manual therapy and the neck involve the VA rather than the ICA.
Deep Dive into Vascular Risk Factors with Roger Kerry
Method Behind The Update
The framework is a consensus document created through a series of robust evidence based stages.
- A survey to evaluate the 2012 framewrok was distributed to all member organisations and special interest groups of IFOMPT in 2016,
- The key issues identified in the survey were initially explored at the IFOMPT conference in 2016. The survey was used to facilitate discussion and the outcome was the need to update the framework. Initial revisions were made after the discussions then SRs and guidelines were used to inform the updated framework and where evidence was not available consensus was used.
- Iterative consultation on the draft was used and circulated to professional member organisations, special interest groups of IFOMPT, international experts as well as osteopaths and chiropractors. The final draft was reviewed by a doctor specialising in stroke and interventinal neurology.
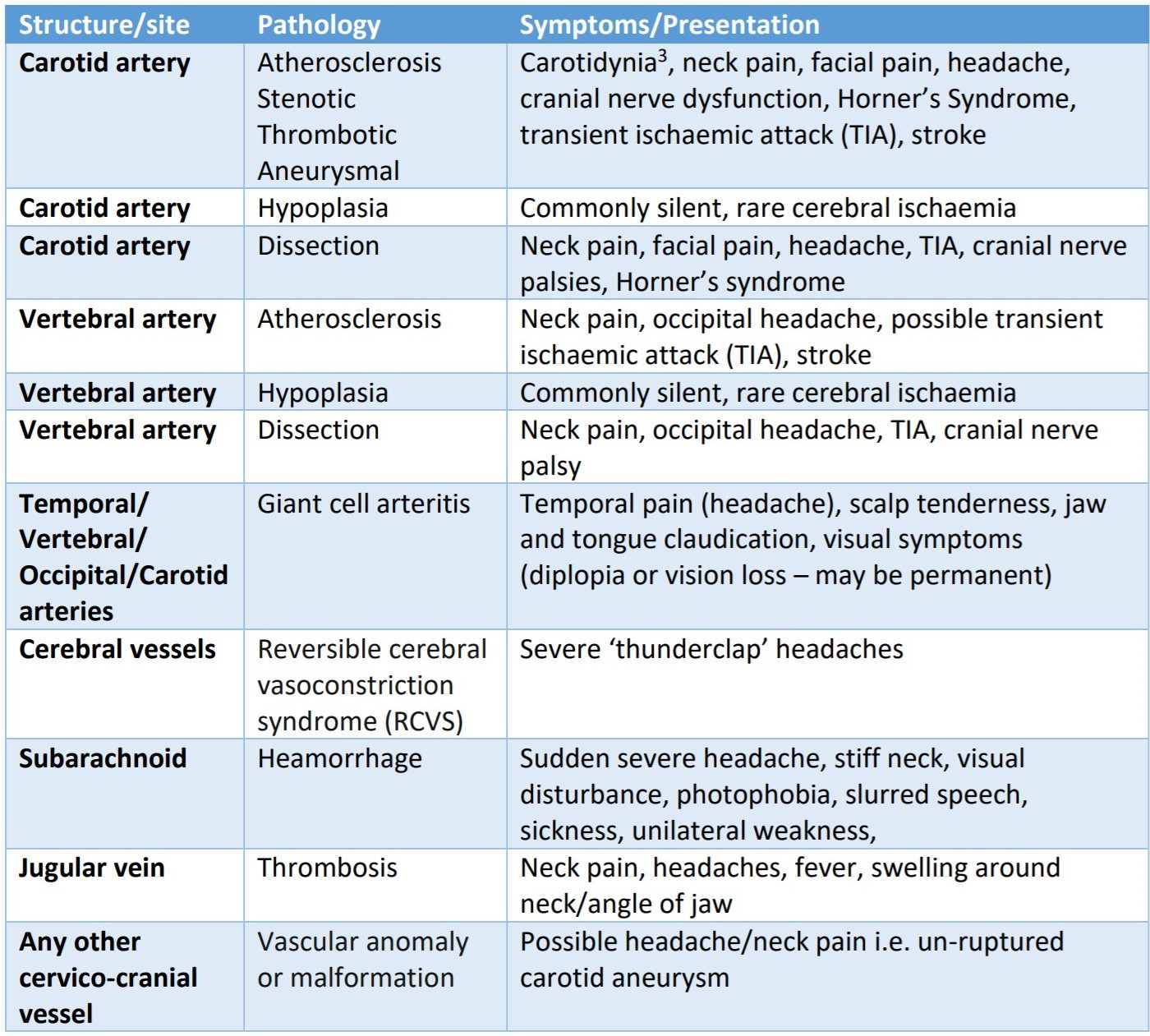
Vascular Pathologies
There are a number of vascular pathologies which all therapist should be aware of, many of which present as musculoskeletal pain. Therefore it is important this is considered within your assessment. The table below is taken directly from the framework document and all information on the pathologies can be found on Physiopedia.
Subjective History & Risk Factors
Rarely is an event associated with a single causal factor, instead they are usually complex and mutifactorial which makes it difficult to know for sure. However there are known risk factors which increase a patients liklihood of having a vascular pathology and therefore contraindicated to manual therapy without further investigation first. These must be known by the clinician and directly drive the liklihood of suspicion.
Definitive tests do not exist as presentations can vary greatly however there are some common features which clinicians should be aware of. Both risk factors and signs as well as symptoms are listed in the infographic below.
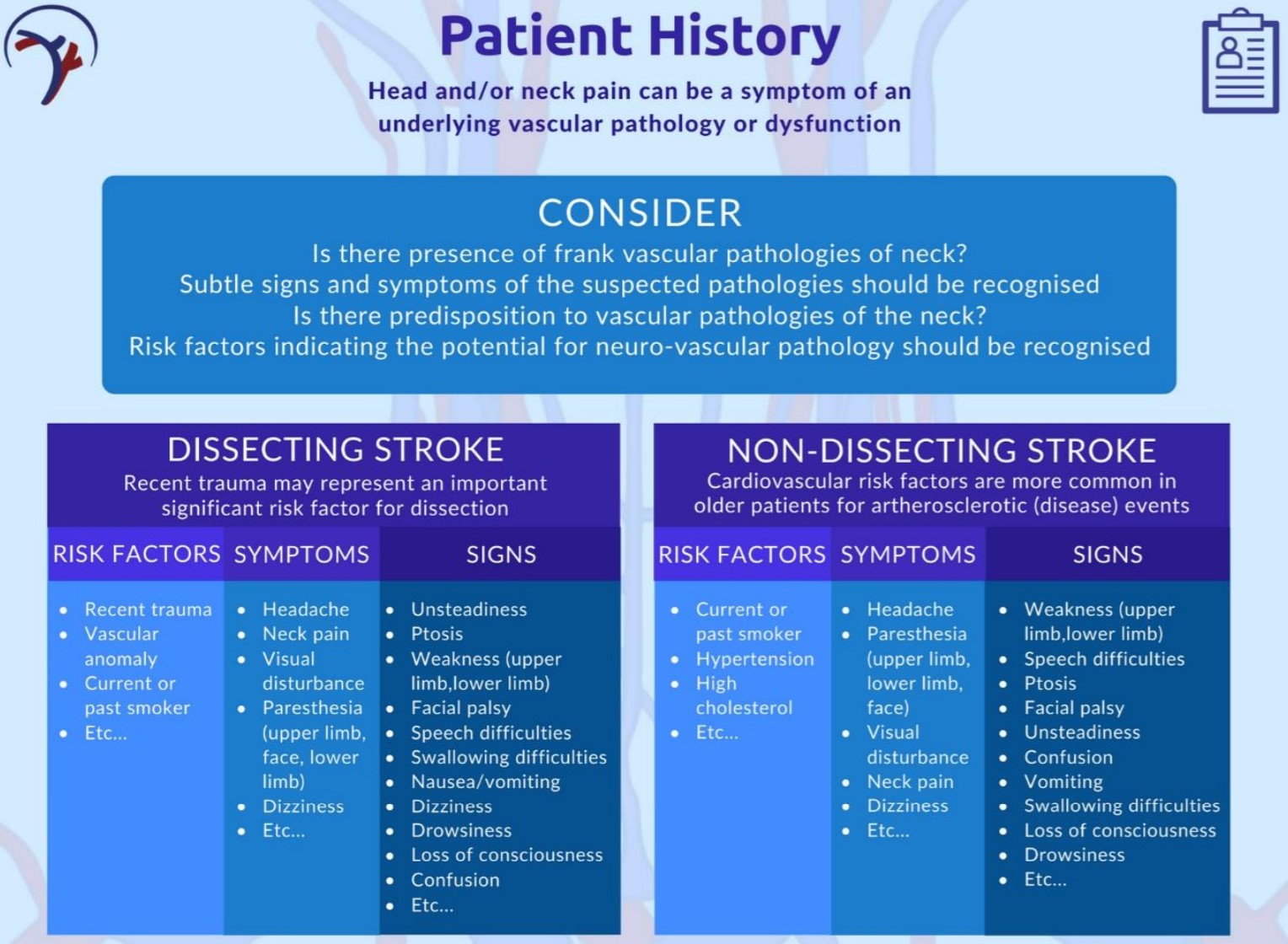
It’s important to remember that spontaneous dissection events are not associated with historical risk factors therefore clinical reasoning must acknowledge that absence of risk factors does not absolutely rule out serious neurovascular event.
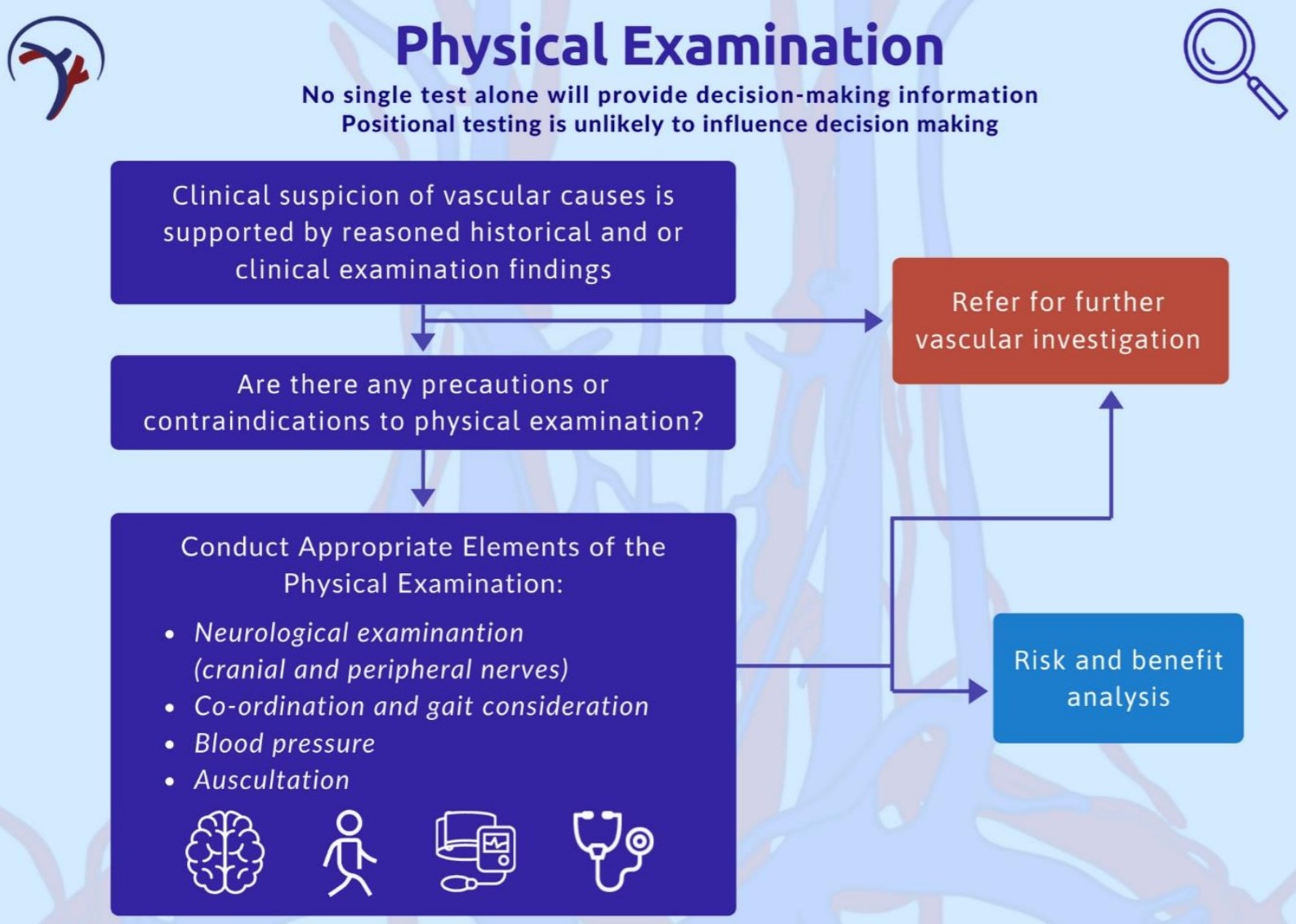
Physical Examination
Always remember the aim of your objective assessment it to test the hypothesis generated in subjective history. The result of the history and examination in the case of of this framework is to establish if an onward referral to a medic is warranted or not. A specific diagnosis is not required rather a decision for a vascular work up or not or to process with physiotherapy intervention.
A key part of the physical examination is establishing a index of suspicion and testing the vascular hypothesis. Three specific examination techniques are
recommended by the framework:
- Blood Pressure
The aim of measuring blood pressure is to assess for risk of stroke and to assess for acute arterial trauma. Hypertension is a strong predictor of CVD however it must be interpreted in the context of other findings. It is also important to remember that there is no discreet threshold rather it is a correlation i.e the higher the BP the higher the risk of vascular pathology. - Neurological examination including cranial nerves
The aim of a neuro examination in this context is to add supporting evidence to your vascular hypothesis. An example of this might be parasthesia or changes in facial sensation which can be a sign of a non-dissecting stroke. Another example might be visual loss with scalp tenderness in giant cell arthritis. - Carotid Artery Examination
This includes both palpatation and auscultation of the carotids. An alteration of pulse has been identified as a feature of internal carotid disease and asymmetry between left and right vessels is considered significant. A pulsatile, expandable mass is indicative of arterial aneurysm. On auscultation a bruit is indicative of a significant finding and should be correlated with the rest of the examaination findings.
Ass with all of the clinical recommendations within the framework there are some info graphics to allow easy digest and reference within clinical practice. The physical examination one is below.
Risk & Benefit
As with all treatment choices risk and benefit need to evaluated. This is particularly important for neck manual therapy for all of the reasons outlines within this article. It is difficult to express the association between risk and benefit as this would require a huge prospective database of hundreds of thousands of patients data. It’s just no feasible. Therefore the assessment of risk and benefit relates to the risk association with treatment, not misdiagnosis.
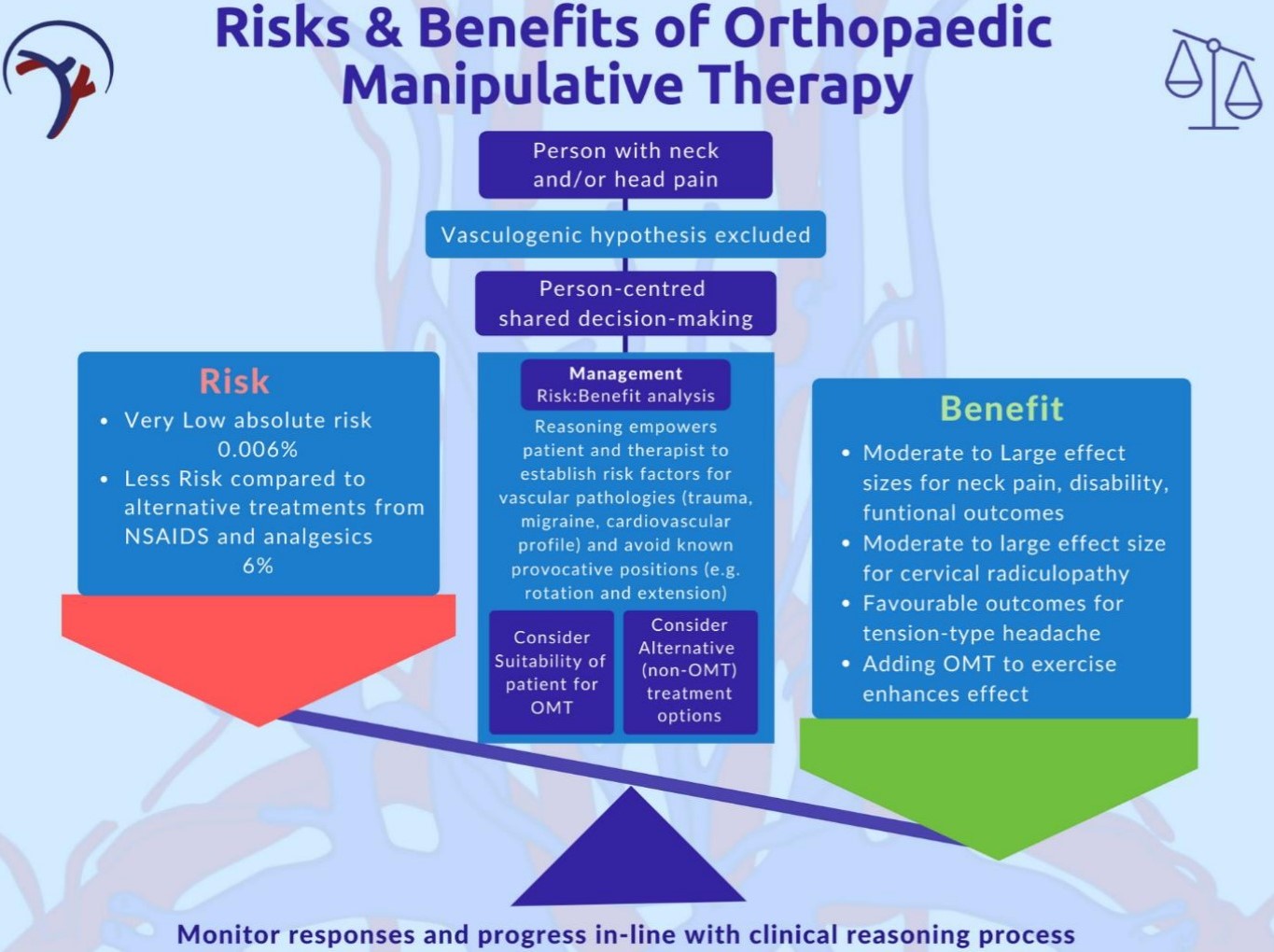
It is the responsibility ot the physiotherapist to recognise and consider whether a patient poses an increased risk and to minimise this. The two major risks are:
- The risk misdiganosis of an existing vascular pathology
- The risk of serious adverse event following manual therapy
The main hypothesis is that the patients presenting with head/neck pain and go on to suffer a serious adverse event i.e dissectionm have an underlying pathology which is aggravated by treatment. It is, therefore, incumbent upon the physical therapist to mitigate such risk by considering known risk factors, signs and symptoms outlined in this Framework in as much as this is possible.
Clinical Reasoning Flow Chart
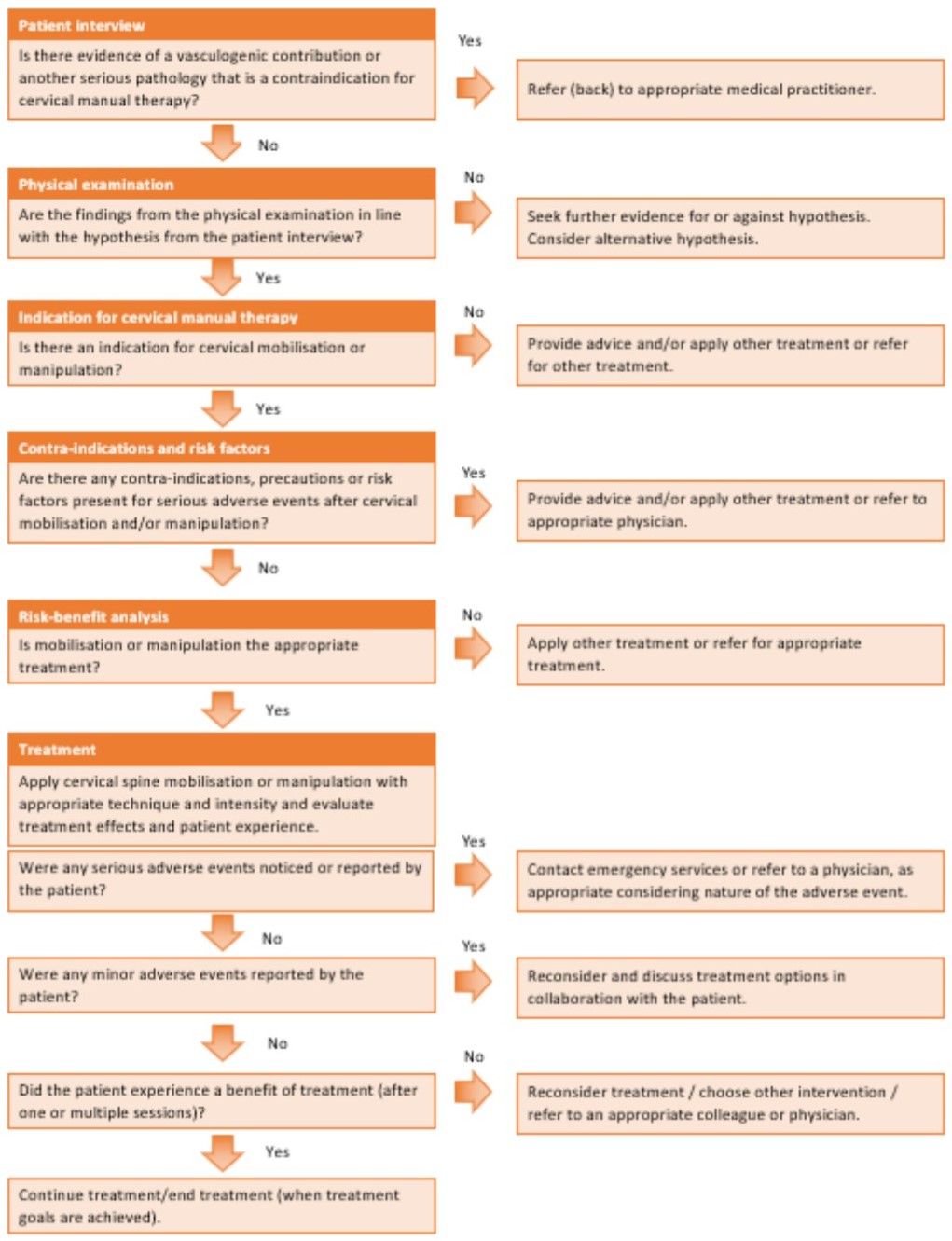
Other Parts of The Framework
The rest of the framework provides details on the following areas:
- Teaching recommendations for instructors
- Medicolegal framework and shared decision making
- What safe manual therapy practice looks like
 Vascular Pathologies of the Neck is term a used in physiotherapy to cover a variety of vascular pathologies which can cause restrictions in blood flow to the brain. When assessing and treating the cervical spine, it is vital to understand diseases of the blood vessels that can present with pain and also to be able to assess the level of risk of a patient experiencing an arterial flow restriction during a physiotherapy assessment or treatment. In this course you will learn from Roger Kerry how to make safe clinical decisions that take into account these very serious issues and how the related framework for clinical practice is being updated.
Vascular Pathologies of the Neck is term a used in physiotherapy to cover a variety of vascular pathologies which can cause restrictions in blood flow to the brain. When assessing and treating the cervical spine, it is vital to understand diseases of the blood vessels that can present with pain and also to be able to assess the level of risk of a patient experiencing an arterial flow restriction during a physiotherapy assessment or treatment. In this course you will learn from Roger Kerry how to make safe clinical decisions that take into account these very serious issues and how the related framework for clinical practice is being updated.